The Shoulder
Infiltrations
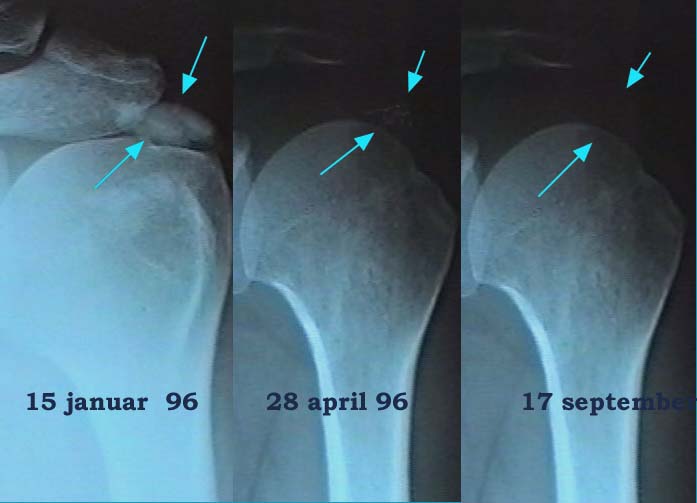
Calcifications
Prevalence
Calcifying tendinitis is a common disorder. Reports on the overall incidence vary between 3 and 7 % of individuals. Most of the calcifications remain symptomless. The supraspinatus tendon is most frequently involved (up to 80% of the cases).
Calcifying tendinitis has a peak incidence in the fifth decade and calcifications are seldom seen in patients older than 70. This means that the 'disorder' is of a self-healing neature and that the various aspects of its pathology are not characteristic of a degenerative disease.
Clinical presentation
The pathogenesis of the disease is unclear but primary degeneration is the most popular theory.
When larger deposits lead to impingement against the acromioclavicular ligament, un uncomplicated calcification hardly causes symptoms, if any at all.
Therefore the first approach is to ignore the calcification and merely treat the tendon itself in the ordinary way, since the lesion pain is usually due to an inflammation adjacent to the calcification and not due to the deposit itself.
It should be remembered that an infiltration with triamcinolone is the treatment of choice and deep transverse frictions is merely contra-indicated in calcifying tendinitis.
If the tendinitis recurs several times one may conclude that the calcification plays a role in the pathogenesis of the tendinitis and an endeavour must be made to get rid of it.
Treatment
- Asymptomatic Calcium deposits are left alone.
- If the tendinitis recurs after initial improvement with a triamcinolone infiltration, the deposit may be held responsible. It should then be considered to dissolve the calcium deposit.
- The site should then be infiltrated with two to five cc 2% procaine hydrochloride once every week until the symptoms cease. Usually two to four infiltrations suffice.
- The first infiltration is done with 10 mg triamcinolone in the mixture, to prevent a potential increase in inflammation. The acid solution of procaine hydrochloride dissolves the deposit which becomes absorbed.
- The technique of infiltration is the same as for a non-calcifying tendinits.
| [Start] | [Main shoulder] | [Flowcharts shoulder] | [A System of Orthopaedic Medicine] |
Copyright © 2021 DR. L. OMBREGT All Rights Reserved
The author can not be held responsible for any damage caused by the use of any information provided.